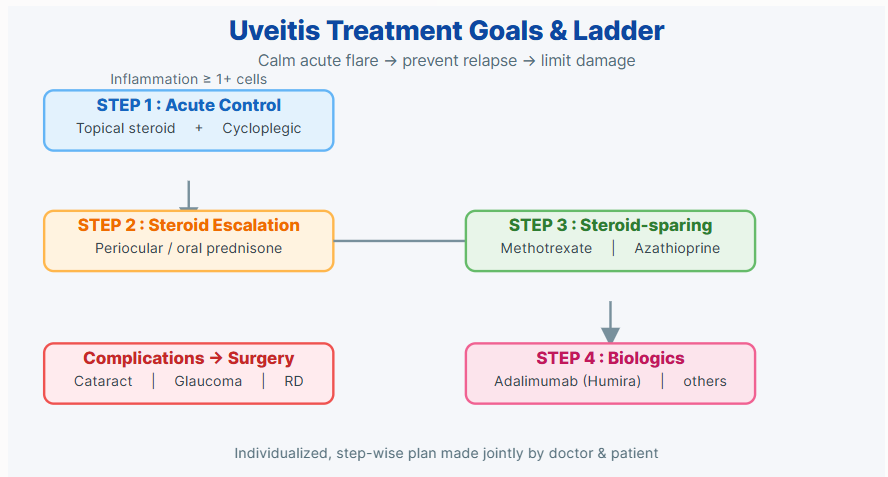
The treatment goals are two: first, to quickly suppress active inflammation—especially when intraocular inflammatory cell count reaches 1+ or higher, it should be controlled in time to prevent further damage; second, to modulate the immune system through immunosuppressants to reduce long-term relapse and tissue destruction risk. Common practices are to first use topical glucocorticoid eye drops and mydriatics, and use systemic glucocorticoids short-term or long-term if necessary; when inflammation needs long-term control or steroid side effects are unacceptable, immunosuppressants (such as methotrexate) or biological agents (such as Humira/adalimumab) are used for difficult cases. If severe complications (such as cataract, glaucoma, or retinal detachment) occur, surgery may also be required. Treatment is a long-term and individualized process, and drug choice, dose and timing will be adjusted by doctors and patients together according to the cause, inflammation activity and complication status. My ophthalmologist found a suitable plan step by step according to these goals.